[Pseudarthrose nach Ruptur einer inkompletten lunotriquetralen Koalition: ein Fallbericht]
Oliver Lotter 1Amro Amr 1
Stephane Stahl 1
Stephan Clasen 2
Christina Schraml 2
Matthias Pfau 1
Hans-Eberhard Schaller 1
1 Department of Plastic, Hand and Reconstructive Surgery, Burn Center, BG Trauma Center, Eberhard-Karls University Tübingen, Germany
2 Department of Diagnostic and Interventional Radiology, Eberhard-Karls University Tübingen, Germany
Zusammenfassung
Während lunotriquetrale Synostosen üblicherweise keine Symptome verursachen, können fibrokartilaginöse Koalitionen ulnarseitige Handgelenksbeschwerden verursachen. Ziel dieser Arbeit ist die Darstellung einer schmerzhaften Pseudarthrose nach traumatischer Läsion einer inkompletten lunotriquetralen Koalition. Des Weiteren sollen Diagnose- und Therapiemöglichkeiten diskutiert werden. Der Fall eines 35-jährigen Mannes wird beschrieben, bei dem die Verletzung einer fibrokartilaginären lunotriquetralen Koalition zur schmerzhaften Pseudarthrose führte. Es erfolgte eine lunotriquetrale Fusion mit Einbringen eines kortikospongiösen Beckenkammspanes und Osteosynthese mittels Herbert-Schraube. Dadurch kam es zur Schmerzfreiheit bei geringgradiger Bewegungseinschränkung. Wir empfehlen die lunotriquetrale Fusion im seltenen Falle einer Fraktur oder Pseudarthrose bei zugrundeliegender lunotriquetraler Koalition. Abhängig von der Größe der Spaltbildung nach Pseudarthrosenresektion sollte die Interposition eines kortikospongiösen Spanes in Erwägung gezogen werden.
Schlüsselwörter
lunotriquetrale Koalition, Pseudarthrose
Introduction
Luno-triquetral coalition is a congenital carpal anomaly that is most often diagnosed as an incidental finding in asymptomatic patients and can be associated with other synostoses or malformations. It is the most common coalition representing nearly 90% of all carpal fusions, followed by the capito-hamate coalition with 5.6% [1]. The prevalence in the general population averages 0.1% but is thought to be 100 times higher in Africans [2]. This anomaly is found more often in females with a ratio of 2:1 [3], [4]. Embryological carpal coalition represents a failure of cavitation of the cartilaginous hand bud precursor during the 4th to 8th week of gestation, which later develops to an osseous, fibrous or cartilaginous union [5]. It is classified according to the degree of union and is often found bilateral. According to literature, the biggest collective has been reported from Senegal, where 32 luno-triquetral coalitions in 20 patients were examined in a retrospective study. The complete form (type III of Minaar's Classification) was the most frequent (46.8%), followed by the incomplete osseous fusion (type II of Minaar's Classification) with a distal notch (28,1%) [6], [7]. Whilst synostosis of the lunate and the triquetrum is known to be asymptomatic, fibro-cartilaginous bonding can present an uncommon cause for ulnar-sided wrist pain [8], [9]. This is the case of a pseudarthrosis after traumatic disruption of a fibro-cartilaginous luno-triquetral coalition type I of Minaar's Classification causing severe wrist pain.
Case presentation
A 35-year-old right-hand dominant white male launderer presented in our policlinic with right-sided wrist pain since 7 months after he had fallen on the same hand. He described an ulno-dorsal intermittent stabbing pain on twisting his hand, particularly when bearing loads. Physical examination revealed tenderness located in the luno-triquetral joint. No swelling or ache in other locations of the right hand could be found. On examination, the left wrist was completely asymptomatic and there was no pathologic “shuck” and “shear” test between the lunate and the triquetrum [10]. The range of motion of the right wrist was 40-0-30 degrees for extension and flexion whereas the left wrist showed no restricted functionality. Plain radiographs showed a right-sided coalition of the lunate and triquetrum (Figure 1 [Fig. 1]), as well as an incomplete fibro-cartilaginous coalition type I on the left side (not shown). Radial and ulnar clenched fist views of both wrists showed no anomaly.

A CT scan of the right wrist revealed a narrowing and irregularity of the proximal luno-triquetral joint space indicating a fibro-cartilaginous coalition type Minaar I which could not be classified in conventional radiographs before (Figure 2 [Fig. 2]).

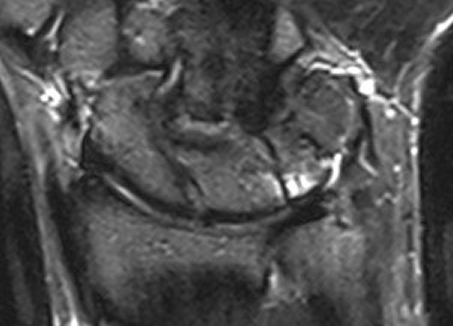
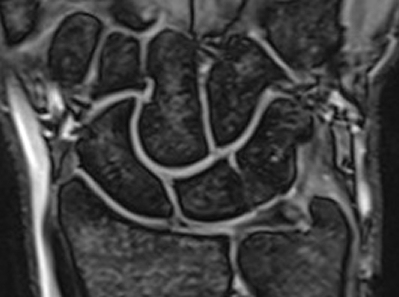
Magnetic Resonance Imaging showed a bone marrow edema adjacent to the fibro-cartilage coalition as well as hyaline cartilage in the distal notch (Figure 3 [Fig. 3], Figure 4 [Fig. 4]).
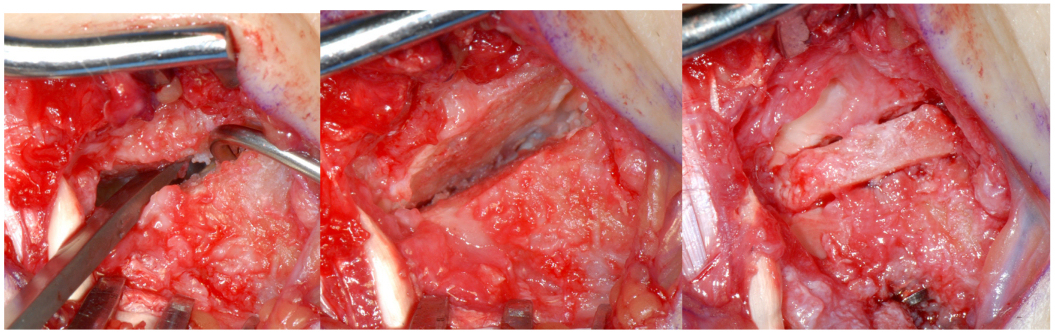
Dynamic fluoroscopy demonstrated a widening of the luno-triquetral region upon ulnar movement and clenching of the wrist. We recommended to fuse the lunate and triquetrum. Using the approach from the 5th extensor tendon compartment, a pseudarthrosis could be visualized and resected (Figure 5 [Fig. 5]). Due to gap formation of approximately 3 millimeters and the inability to approximate the bones without tension, we decided to make use of a corticocancellous wedge from the iliac crest (Figure 6 [Fig. 6]). A 24-millimeter Herbert screw was used for stabilization. Immobilization was continued until 6 weeks after the operation. Plain radiographs and a CT scan after this time showed an advanced bony consolidation with the Herbert screw in correct position and length. The patient still suffered from some swelling of the hand. Range of motion was 30-0-10 degrees for wrist extension/flexion and 70-0-90 degrees for supination/pronation of the forearm. At this stage we discontinued immobilization of the wrist and the patient began with exercises without loading. Three months after luno-triquetral fusion the patient was almost painless and range of motion had improved to 40-0-40 degrees for wrist extension/flexion. Plain radiographs showed bony consolidation. Another CT-scan was planned at 6 months after the intervention.

Discussion
The joint between lunate and triquetrum is the most common location for carpal coalition. Depending on the degree of cellular apoptosis, different types of bonding can develop, which can range anywhere between complete coalition or normal joint development. Minaar classified this anatomical variation in 4 types. Type I represents an incomplete fusion with a strong fibro-cartilaginous component, type II an incomplete osseous fusion, type III a complete osseous fusion (os lunato-triquetrum) and type IV a complete osseous fusion associated with other carpal anomalies [7], [11].
Whilst some authors believe that all types of luno-triquetral bonding are asymptomatic, others differentiate Minaar's type I conditions from the bony coalitions of Minaar's type II–IV. To their opinion, fibro-cartilaginous coalitions are likely to cause wrist pain [3]. Fractures of osseous coalitions have been reported. However these might have been symptomatic fibrocartilaginous situations as suggested by Resnik et al. [9]. For proper diagnosis we suggest to perform anterior-posterior and lateral radiographs as well radial and ulnar clenched fist views of both wrists. Scapho-lunate joint space widening is commonly associated with luno-triquetral coalition but was not present in our case [12]. Cineradiography can be added if abnormal motion of the carpal bones in relation to each other is suspected. We recommend a CT scan in case of difficulty evaluating the stability of the bonding between the affected carpal bones in symptomatic wrists. To our opinion the only reasons to justify Magnetic Resonance Imaging are to exclude concomitant pathologies of the wrist and to gain some information about the condition of articular cartilage in incomplete luno-triquetral coalition. Only 6 cases of disrupted luno-triquetral coalitions have been described in literature, three of which were treated operatively using K-wires or a screw [3], [8], [13], [14], [15], [16]. In our patient gap formation occurred after resection of the luno-triquetral pseudarthrosis and the carpal bones could not be approximated without tension. In such a case we strongly recommend the use of a corticocancellous wedge to avoid alteration of the carpal framework and the translation of carpal bones to each other. This is the first time to describe a technique which is usually applied for treatment of scaphoid non-union with a favourable outcome in luno-triquetral coalition.
Conclusion
We recommend limited carpal fusion in symptomatic fracture or pseudarthrosis of luno-triquetral coalition. If gap formation after resection of the pseudarthrosis is present, a corticocancellous wedge should be interposed.
Notes
Conflicts of interest
The authors disclose the absence of any conflict of interest following the guidelines of the International Committee of Medical Journal Editors.
References
[1] Delaney TJ, Eswar S. Carpal coalitions. J Hand Surg Am. 1992;17(1):28-31. DOI: 10.1016/0363-5023(92)90108-2[2] Cockshott WP. Carpal fusions. Am J Roentgenol Radium Ther Nucl Med. 1963;89:1260-71.
[3] Simmons BP, McKenzie WD. Symptomatic carpal coalition. J Hand Surg Am. 1985;10(2):190-3.
[4] Garn SM, Frisancho AR, Poznanski AK, Schweitzer J, McCann MB. Analysis of triquetral-lunate fusion. Am J Phys Anthropol. 1971;34(3):431-3. DOI: 10.1002/ajpa.1330340313
[5] Moore KI. Embryology of the hand. In: Herndon DN, editor. The Developing Human. Philadelphia: WB Saunders; 1988. p. 355-7.
[6] Sy MH, Diarra O, Diagne M, Diouf MM, Sene P, Diouf S. La synostose pyramido-lunaire chez le noir africain. A propos de trente-deux cas. [Pyramido-lunar fusion in black Africans. Apropos of 32 cases]. Ann Radiol (Paris). 1996;39(4-5):208-12.
[7] Devilliers Minaar AB. Congenital fusion of the lunate and triquetral bones in the South African Bantu. J Bone Joint Surg Br. 1952;34-B(1):45-8.
[8] Van Schoonhoven J, Prommersberger KJ, Schmitt R. Traumatic disruption of a fibrocartilage lunate-triquetral coalition: a case report and review of the literature. Hand Surg. 2001;6(1):103-108. DOI: 10.1142/S0218810401000497
[9] Resnik CS, Grizzard JD, Simmons BP, Yaghmai I. Incomplete Carpal Coalition. AJR Am J Roentgenol. 1986;147(2):301-4.
[10] Kleinman WB. Distal ulnar injury and dysfunction. Indiana Hand Center Newslett. 1995;2:7-17
[11] Ritt MJ, Maas M, Bos KE. Minaar type 1 symptomatic lunotriquetral coalition: a report of nine patients. J Hand Surg Am. 2001;26(2):261-70. DOI: 10.1053/jhsu.2001.21520
[12] Metz VM, Schimmerl SM, Gilula LA, Viegas SF, Saffar P. Wide scapholunate joint space in lunotriquetral coalition: a normal variant? Radiology. 1993;188(2):557-9.
[13] McGoey PF. Fracture-dislocation of a fused triangular and lunate (congenital). J Bone Joint Surg. 1943;25:928-9.
[14] Auerbach DM, Collins ED. An unusual fracture dislocation pattern in a patient with an os lunatotriquetrum. Am J Orthop (Belle Mead NJ). 1995;24(9):714-6.
[15] Peyton RS, Moore RJ. Fracture through a congenital carpal coalition. J Hand Surg Am. 1994;19(3):369-71. DOI: 10.1016/0363-5023(94)90047-7
[16] Laurencin CT, Cummings RS, Jones TR, Martin L. Fracture-dislocation of the luno-triquetral coalition. J Natl Med Assoc. 1998;90(12):779-81.

