Adult posterior urethral valve: a case report
Mete Kilciler 1Seref Basal 1
Hasan Cem Irkilata 1
Murat Zor 1
Mustafa Okan Istanbulluoglu 1
Murat Dayanc 1
1 Gülhane Military Medical Academy, Department of Urology, Kecioren, Ankara, Turkey
Abstract
Introduction: Posterior urethral valve (PUV) is a congenital obstructive defect of the male urethra with an incidence of 1/8,000 to 1/25,000 live births. PUV is the most common cause of lower urinary tract obstruction in neonates. The diagnosis of PUV is usually made early, and PUV cases have rarely been detected in adults.
Case presentation: Here we report the case of a 35 years old man presented with obstructive urinary symptoms. In spite of bladder neck rejection uroflowmetry pointed out infravesical obstruction with max. flow rate 9 ml/s and average flow rate 6 ml/s in uroflowmetry. During cystoscopy mild bladder trabeculation and resected bladder neck were seen. While the cystoscope was taken off, PUV were obtained.
Conclusion: Since PUV is a rare condition in adults and the diagnosis of PUVs is also difficult in these groups we must consider this situation during evaluation of adult patients with obstructive symptoms especially during cystourethroscopy.
Keywords
urethral obstruction, adult, posterior urethral valve
Introduction
Posterior urethral valve (PUV) with an incidence of 1/8.000 to 1/25.000 live births is the most common cause of lower urinary tract obstruction in male neonates [1], [2]. This pathology constitutes a clinical spectrum ranging from severe forms, with important repercussions on the upper urinary tract and renal function (RF), to milder forms [3], [4], [5]. When obstruction can be overcome by detrusor contraction it may remain silent until later life [1], [2]. The majority of cases are diagnosed in infancy and early childhood especially during evaluation of male newborn for prenatal hydronephrosis and rarely in adolescence or adulthood. The diagnosis of PUV is usually made early, and PUV cases have rarely been detected in adults [6], [7], [8], [9]. Here we report the case of a 35-year-old man with PUV, who presented with obstructive symptoms.
Case presentation
A 35 years old male patient presented with lower urinary tract symptoms for a long time. His complaints increased for the last two years. Because of this symptoms, transurethral bladder neck resection was performed one year ago, but his symptoms did not disappear. Biochemical analysis, hemogram and urinalysis were normal and urine culture was sterile. Sonography of kidney, bilateral ureter, bladder and prostate were normal. Uroflowmetry pointed out infravesical obstruction with max. flow rate 9 ml/s and average flow rate 6 ml/s. Postvoid residual urine was measured 60 ml by bladder scan. We performed cystourethroscopy to find out the reason of obstruction. During cystourethroscopy mild bladder trabeculation and resected bladder neck were seen. At the beginning we could not find any urethral pathology. After filing bladder we inspected the urethra, while taking out the cystoscope, PUV was incidentally determined (Figure 1 [Fig. 1]). In order to verify if it was true PUV or urethral folding, valves were hooked with Collins knife (Figure 2 [Fig. 2], Figure 3 [Fig. 3]). Patient symptoms disappeared and complete emptying of the bladder were determined after 3 months of operation, with normal voiding pattern and max. flow rate 16 ml/s and average flow rate 10 ml/s in uroflowmetry. No postvoid residual urine was detected.
Figure 1: Endoscopic view of posterior urethral valve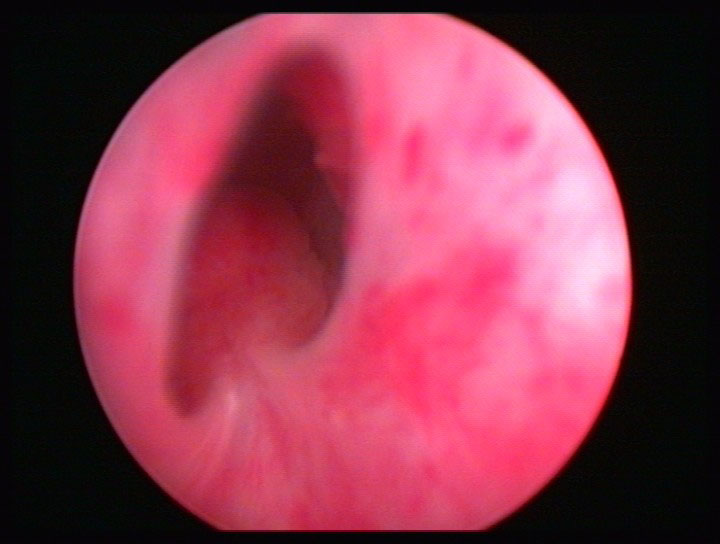
Figure 2: Ablation of posterior urethral valve with Collins knife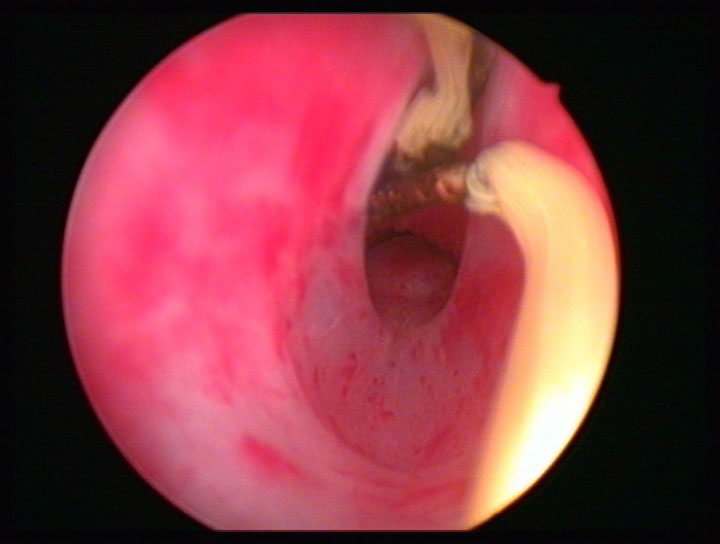
Figure 3: Endoscopic view of urethra after ablation of posterior urethral valve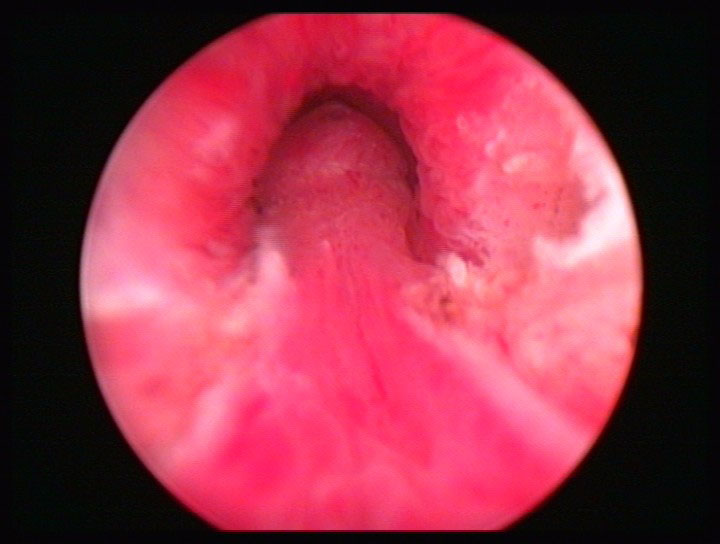
Discussion
PUVs are the commonest cause of obstruction in neonates, when obstruction can be overcome by detrusor contraction it may remain silent until later life [1], [2]. The exact age of presentation is not known and varies greatly. PUVs usually detected in infants are more severe than in adults. Symptoms leading to the diagnosis include irritative symptoms of the lower urinary tract, recurrent urinary infections, obstructive symptoms, and, rarely, ejaculation diseases, gross haematuria, and renal insufficiency [6], [8]. Voiding cystourethrography (VCUG) is the definitive radiographic study. In our case we made the diagnosis and the treatment simultaneously during cystourethroscopy, thus we did not perform VCUG.
Fibrous bladder neck contracture occurred in 76% of adults, and its incidence has been correlated with patient age [6]. Some investigators have suggested that high prostatic pressure leads to sclerosing prostatitis and often to gradual fibrosis of the bladder neck. Bladder neck incision is recommended in the case of persistent obstruction after resection of PUVs or during PUV resection in the case of severe stricture in adults only [10]. In this case the patient had bladder neck rejection before detection of PUV. Since his symptoms persisted after bladder neck rejection, cystourethroscopy was performed and after careful examination of urethra PUV was determined and valves were hooked with Collins knife.
Since PUV is a rare condition in adults and the diagnosis of PUV is also difficult in these groups we must consider this situation during evaluation of adult patients with obstructive symptoms especially during cystourethroscopy. When a bladder neck fibrosis is observed during cystourethroscopy in adult patients with obstructive symptoms, urethroscopy shall eliminate PUV.
Notes
Consent
Written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal. The patient permitted to have his cystoscopy images published.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SB analyzed and interpreted the patient data, HCI took part in the critical revision, MK and MD took part in the surgical approach, MOI and MZ drafted the article and SB took part in final approval of the manuscript.
All authors read and approved the final manuscript.
References
[1] Atwell JD. Posterior urethral valves in the British Isles: A multicenter BAPS review. J Pediatr Surg. 1983;18(1):70-4. DOI: 10.1016/S0022-3468(83)80276-0[2] Opsomer RJ, Wese FX, Dardenne AN, Van Cangh PJ. Posterior urethral valves in adults males. Urology. 1990;36(1):35-7. DOI: 10.1016/0090-4295(90)80309-B
[3] Dinneen MD, Duffy PG. Posterior urethral valves. Br J Urol. 1996;78(2):275-81.
[4] Hendren WH. Posterior urethral valves in boys: a broad clinical spectrum. J Urol. 1971;106(2):298-302.
[5] Denes ED, Barthold JS, Gonzalez R. Early prognostic value of serum creatinine levels in children with posterior urethral valves. J Urol. 1997;157(4):1441-3. DOI: 10.1016/S0022-5347(01)65015-8
[6] Mahony T, Laferte RO. Congenital posterior urethral valves in adult males. Urology. 1974;3(6):724-34. DOI: 10.1016/S0090-4295(74)80214-1
[7] Saraf PG, Valvo JR, Frank IN. Congenital posterior urethral valves in an adult. Urology. 1984;23(1):55-7. DOI: 10.1016/0090-4295(84)90177-8
[8] Páramo PG, Martinez-Piñeiro JA, De La Peña JJ, Páramo PS Jr. Andrological implications of congenital posterior urethral valves in adults: a case of retained ejaculation and review in Western literature. Eur Urol. 1983;9(6):359-61.
[9] Köksal IT, Usta M, Erdog(ru T, Ates, M, Kukul E, Baykara M. Incidental adult posterior urethral valve without clinical features. Int Urol Nephrol. 2003;35(2):227-9.
[10] Culty T, Delongchamps NB, Dominique S, Servin F, Ravery V, Boccon-Gibod L. Posterior urethral valves in adult with Down syndrome. Urology. 2006;67(2):424.e1-424.e2.

