Subcutaneous lateral brow lift (“Z-lift”)
Klaus Ueberreiter 1Ursula Tanzella 1
Yves Surlemont 2
Björn Dirk Krapohl 3,4
1 Park-Klinik Birkenwerder, Germany
2 Clinique Saint-Antoine, Rouen, France
3 Department of Plastic and Hand Surgery, St. Marien-Krankenhaus Berlin, Germany
4 Charité – Medical University of Berlin, Germany
Abstract
Surgical eyebrow lift has been described by using many different open and endoscopic methods. Difficult techniques and only short time benefits oft lead to patients’ complaints. We present a safe and simple temporal Z-incision technique for eyebrow lift in 37 patients. Besides simplicity and safety, our technique shows long lasting aesthetic results with hidden scars and a high rate of patient satisfaction.
Keywords
brow lift, aesthetic surgery, facial surgery
Introduction
For many years, endoscopic forehead lift was the preferred tool and a plastic surgeon’s hand. But in many cases the position of the eyebrows especially in the medial part was relocated far too high. In a youthful appearance, usually the medial part of the brows is quite small as the lateral part is directed more upwards [1], [2], [3], [4], [5], [6].
Many patients who ask for an upper eyelid surgery show signs of lowered lateral brows.
We developed a technique to lift those brows in a very easy and reliable way with excellent control of the appropriate vector with the necessity of basic instrument use only.
Material and method
Since 2012 we have established the Z-lift routine procedure, meanwhile introduced in about one third of all our brow lifts. So far 37 patients have been evaluated.
The procedures were usually combined with an upper eyelid blepharoplasty and also with facelift procedures, hence avoiding a cranial scar extension.
Only in 13 cases the Z-lift was performed as a stand-alone procedure. The effect of the lift was measured by photographic means six months after the operation. Patients were also asked about their satisfaction with the results.
Planning of operation
Before the intervention the vector of the planned brow lift is checked by pulling up the skin with one hand. The patient is invited to check the effect in the mirror. The resulting vector ranges between 30 and 70°. The vector line is drawn crossing the temporal hairline and a few centimetres behind this hairline, above the temporal muscle, a rectangular line is drawn to reside in a cross (Figure 1 [Fig. 1]).
Figure 1: Marking of the vector for the eyebrow elevation
The arms of this cross will be limited by markings to each one 1 cm length. In this way a shape like a small hourglass is created (Figure 2 [Fig. 2]).
Figure 2: Marking of the hourglass shaped skin excision posterior to the hair line
Operation
The operation can be done under local anaesthesia, sedation, or general anaesthesia according to the patient’s and surgeon’s choice.
The area around the hourglass drawing, along the vector, up to the medial part of the brows, going well to the lateral hairline and below the “crow’s feet” is infiltrated with local anaesthetic and epinephrine, usually about 30 to 40 ml per side. In the next step the complete excision of the upper and lower triangle of the hourglass is performed (Figure 3 [Fig. 3], Figure 4 [Fig. 4]), followed by incision along the line crossing the vector down to the space between the outer and inner sheet of the temporal muscle facia. The preparation follows this open space for roughly 1 cm in direction to the brows. Then a sharp hook is placed to elevate the skin with the adherent superficial fascia, and using a small blade, this fascia is cut in a semi-circular way to open up again the subcutaneous layer (Figure 5 [Fig. 5]).
Figure 3: Temporal region after skin excision
Figure 4: Resected skin, two triangular full thickness slides per side
Figure 5: Temporo-frontal dissection, beginning strictly under the superficial temporalis fascia
The preparation now follows exactly in the subcutaneous area until well below the brows and the lateral wrinkles.
The preparation should be carried out carefully to preserve the perforating vessels in the central part of the brows. It is finished, when an upward pull in the cross area easily lifts the whole undermined area.
In the upper part now some centimetres in cranial direction on top of the lower temporal fascia are mobilized. The fascial patch adherent to the skin is now pulled up and attached with two 2-0 Vicryl sutures to the deep temporal fascia, cranially to the cross incision (Figure 6 [Fig. 6]).
Figure 6; The actual brow elevation is achieved by a vicryl suture attaching the temporalis fascia flap cranially.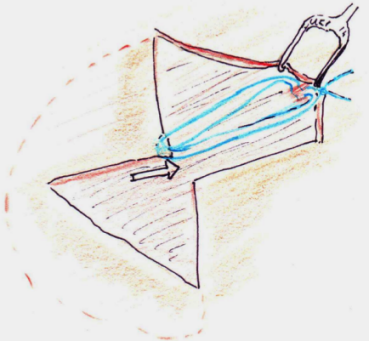
The brow is now lifted in a way that looks overdone, but within the next 3 to 4 weeks it will regain natural appearance. This over-correction is necessary to maintain a good permanent result. For skin closure we use staples. If still some bleeding occurs, a strip of latex or silicone can be inserted as a little drainage. Before applying the dressings, haematoma can be squeezed out and then immediately afterwards an elastic circular compression bandage is applied. This will be left in place for two days. The staples can be removed after 10 days.
Results
32 of our 37 patients rated the result as very satisfying or satisfying, three patients were disappointed with the amount of brow lift, and one was complaining about the small local baldness. Transient paralysis of the frontal branch of the facial nerve was observed in three patients. It resolved after 3 to 6 months and did not lead to complaints, because the brows are well attached in their new cranial position and the folds of the forehead had disappeared on the concerned side. The problem is always the over-reacting contralateral side which leads to an asymmetric appearance. This can be easily treated by injections of botulinum toxin.
Immediate post-operative haematoma occurred in five cases and could easily be resolved. With the learning curve of the surgeon this complication becomes very rare.
We present clinical examples of our results, see Figure 7 [Fig. 7] and Figure 8 [Fig. 8].
Figure 7: Patient one year after lateral Z-brow lift
Figure 8: Patient 10 months after Z-brow lift
Discussion
There are several common methods of eyebrow lift. The easiest approach is direct excision of skin above the brow line [7], [8], [9], [10], [11]. Another method is the approach via the blepharoplasty. The disadvantage hereby is the merely moderate short-time elevation of the brow.
The most common approach is the endoscopic lateral brow lift [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24]. The disadvantage of this procedure is difficult stable anchoring and the complexity of the setup. Subcutaneous approaches have been described before [25], [26], [27], [28], [29]. We have developed a variation, which avoids the relatively long incision line above the temporal muscle and results only in a barely visible short zigzag scar (Figure 9 [Fig. 9]).
Figure 9: The scar is barely visible after 8 weeks and hidden behind the hair line.
The main advantage of our method lies in the easy planning and in the versatility of the applied vector lines in comparison to the traditional temporal sub-fascial brow lift. The incidence of publications about anchor systems shows a necessity for a reliable technique, if possible, just using re-absorbable simple sutures [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [41]. In the subcutaneous layers, we expect a far better long time adhesion compared to the sub-fascial plane. The subcutaneous fascial patch is an excellent anchor place to allow for a strong upward pull with simple Vicryl sutures, thus avoiding problems arising from very slow re-absorbable or non-absorbable materials. The third positive aspect is a safe preparation strictly above the temporal branch of the facial nerve [42], [43], [44].
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Freund RM, Nolan WB 3rd. Correlation between brow lift outcomes and aesthetic ideals for eyebrow height and shape in females. Plast Reconstr Surg. 1996 Jun;97(7):1343-8. DOI: 10.1097/00006534-199606000-00003[2] Roth JM, Metzinger SE. Quantifying the arch position of the female eyebrow. Arch Facial Plast Surg. 2003 May-Jun;5(3):235-9. DOI: 10.1001/archfaci.5.3.235
[3] Feser DK, Gründl M, Eisenmann-Klein M, Prantl L. Attractiveness of eyebrow position and shape in females depends on the age of the beholder. Aesthetic Plast Surg. 2007 Mar-Apr;31(2):154-60. DOI: 10.1007/s00266-006-0149-x
[4] Sclafani AP, Jung M. Desired position, shape, and dynamic range of the normal adult eyebrow. Arch Facial Plast Surg. 2010 Mar-Apr;12(2):123-7. DOI: 10.1001/archfacial.2010.17
[5] Patil SB, Kale SM, Jaiswal S, Khare N, Math M. Effect of aging on the shape and position of the eyebrow in an Indian population. Aesthetic Plast Surg. 2011 Dec;35(6):1031-5. DOI: 10.1007/s00266-011-9728-6
[6] Yalçınkaya E, Cingi C, Söken H, Ulusoy S, Muluk NB. Aesthetic analysis of the ideal eyebrow shape and position. Eur Arch Otorhinolaryngol. 2014 Oct 28. DOI: 10.1007/s00405-014-3356-0
[7] Booth AJ, Murray A, Tyers AG. The direct brow lift: efficacy, complications, and patient satisfaction. Br J Ophthalmol. 2004 May;88(5):688-91. DOI: 10.1136/bjo.2003.019232
[8] Kurlander DE, Collins AB, Bordeaux JS. Direct brow lift after Mohs-induced temporal nerve transection. Dermatol Surg. 2013 Jul;39(7):1132-4. DOI: 10.1111/dsu.12203
[9] Rafaty FM, Goode RL, Fee WE Jr. The brow-lift operation. Arch Otolaryngol. 1975 Aug;101(8):467-8. DOI: 10.1001/archotol.1975.00780370009004
[10] Tyers AG. Brow lift via the direct and trans-blepharoplasty approaches. Orbit. 2006 Dec;25(4):261-5. DOI: 10.1080/01676830600977384
[11] Walrath JD, McCord CD. The open brow lift. Clin Plast Surg. 2013 Jan;40(1):117-24. DOI: 10.1016/j.cps.2012.06.002
[12] Biggs TM. Endoscopic brow lift: a retrospective review of 628 consecutive cases over 5 years. Plast Reconstr Surg. 2004 Jun;113(7):2219; author reply 2219-20.
[13] Bruck JC, Middelberg T. Die endoskopische Brauenanhebung mit resorbierbaren Hautankern [Endoscopic brow lift with resorbable anchors]. Handchir Mikrochir Plast Chir. 2007 Jun;39(3):197-200. DOI: 10.1055/s-2007-965020
[14] Chiu ES, Baker DC. Endoscopic brow lift: a retrospective review of 628 consecutive cases over 5 years. Plast Reconstr Surg. 2003 Aug;112(2):628-33. DOI: 10.1097/01.PRS.0000071042.11435.2E
[15] Ducic Y, Adelson R. Use of the endoscopic forehead-lift to improve brow position in persistent facial paralysis. Arch Facial Plast Surg. 2005 Jan-Feb;7(1):51-4. DOI: 10.1001/archfaci.7.1.51
[16] Fisher O, Zamboni WA. Endoscopic brow-lift in the male patient. Arch Facial Plast Surg. 2010 Jan-Feb;12(1):56-9. DOI: 10.1001/archfacial.2009.109
[17] Graf RM, Tolazzi AR, Mansur AE, Teixeira V. Endoscopic periosteal brow lift: evaluation and follow-up of eyebrow height. Plast Reconstr Surg. 2008 Feb;121(2):609-16. DOI: 10.1097/01.prs.0000298111.56163.3b
[18] Nassif PS. Endoscopic brow-lift with deep temporal fixation only (DTFO). Facial Plast Surg Clin North Am. 2006 Aug;14(3):203-11. DOI: 10.1016/j.fsc.2006.04.004
[19] Nassif PS. Evolution in techniques for endoscopic brow lift with deep temporal fixation only and lower blepharoplasty-transconjunctival fat repositioning. Facial Plast Surg. 2007 Feb;23(1):27-42. DOI: 10.1055/s-2007-970130
[20] Niamtu J 3rd. Endoscopic brow and forehead lift: a case for new technology. J Oral Maxillofac Surg. 2006 Jul;64(7):1129-32. DOI: 10.1016/j.joms.2006.03.041
[21] Panella NJ, Wallin JL, Goldman ND. Patient outcomes, satisfaction, and improvement in headaches after endoscopic brow-lift. JAMA Facial Plast Surg. 2013 Jul-Aug;15(4):263-7. DOI: 10.1001/jamafacial.2013.924
[22] Punthakee X, Mashkevich G, Keller GS. Endoscopic forehead and brow-lift. Facial Plast Surg. 2010 Aug;26(3):239-51. DOI: 10.1055/s-0030-1254335
[23] Terella AM, Wang TD. Technical considerations in endoscopic brow lift. Clin Plast Surg. 2013 Jan;40(1):105-15. DOI: 10.1016/j.cps.2012.06.004
[24] Tower RN, Dailey RA. Endoscopic pretrichial brow lift: surgical indications, technique and outcomes. Ophthal Plast Reconstr Surg. 2004 Jul;20(4):268-73. DOI: 10.1097/01.IOP.0000131734.19609.15
[25] Bernard RW, Greenwald JA, Beran SJ, Morello DC. Enhancing upper lid aesthetics with the lateral subcutaneous brow lift. Aesthet Surg J. 2006 Jan-Feb;26(1):19-23. DOI: 10.1016/j.asj.2005.12.006
[26] Mahmood U, Baker JL Jr. Lateral Subcutaneous Brow Lift: Updated Technique. Aesthet Surg J. 2015 Jul;35(5):621-4. DOI: 10.1093/asj/sju116
[27] Miller TA. Lateral subcutaneous brow lift. Aesthet Surg J. 2003 May;23(3):205-10. DOI: 10.1067/maj.2003.43
[28] Niamtu J 3rd. The subcutaneous brow- and forehead-lift: a face-lift for the forehead and brow. Dermatol Surg. 2008 Oct;34(10):1350-62. DOI: 10.1111/j.1524-4725.2008.34288.x
[29] Pollock H, Pollock TA. Subcutaneous brow lift with precise suture fixation and advancement. Aesthet Surg J. 2007 Jul-Aug;27(4):388-95. DOI: 10.1016/j.asj.2007.05.011
[30] Badin AZ, Bittencourt LM, Balderrama CR. Lateral brow fixation in endoscopic forehead lift: long-term results with braided nylon percutaneous sutures. Aesthetic Plast Surg. 2010 Feb;34(1):78-87. DOI: 10.1007/s00266-009-9401-5
[31] Chasan PE, Kupfer DM. Direct K-wire fixation technique during endoscopic brow lift. Aesthetic Plast Surg. 1998 Sep-Oct;22(5):338-40. DOI: 10.1007/s002669900213
[32] Foustanos A. Suture fixation technique for endoscopic brow lift. Semin Plast Surg. 2008 Feb;22(1):43-9. DOI: 10.1055/s-2007-1019142
[33] Foustanos A, Drimouras G, Panagiotopoulos K. Lateral Brow Lift: A Multi-Point Suture Fixation Technique. Arch Plast Surg. 2015 Sep;42(5):580-7. DOI: 10.5999/aps.2015.42.5.580
[34] Foustanos A, Zavrides H. An alternative fixation technique for the endoscopic brow lift. Ann Plast Surg. 2006 Jun;56(6):599-604. DOI: 10.1097/01.sap.0000203317.50871.5c
[35] Gold AH, Bernard RW, Hamas RS, McKinney P, Paul MD. Brow lift fixation. Aesthet Surg J. 2003 May;23(3):217-9. DOI: 10.1067/maj.2003.55
[36] Kobienia BJ, Van Beek A. Calvarial fixation during endoscopic brow lift. Plast Reconstr Surg. 1998 Jul;102(1):238-40. DOI: 10.1097/00006534-199807000-00040
[37] Malata CM, Abood A. Experience with cortical tunnel fixation in endoscopic brow lift: the "bevel and slide" modification. Int J Surg. 2009 Dec;7(6):510-5. DOI: 10.1016/j.ijsu.2009.08.013
[38] Mavrikakis I, DeSousa JL, Malhotra R. Periosteal fixation during subperiosteal brow lift surgery. Dermatol Surg. 2008 Nov;34(11):1500-6. DOI: 10.1111/j.1524-4725.2008.34313.x
[39] McKinney P, Celetti S, Sweis I. An accurate technique for fixation in endoscopic brow lift. Plast Reconstr Surg. 1996 Apr;97(4):824-7. DOI: 10.1097/00006534-199604000-00022
[40] Mutaf M. Mesh lift: a new procedure for long-lasting results in brow lift surgery. Plast Reconstr Surg. 2005 Oct;116(5):1490-9. DOI: 10.1097/01.prs.0000182601.94805.58
[41] Pascali M, Avantaggiato A, Bocchini I, Carinci F, Cervelli V. Comparison among three different fixation techniques in temporal brow lift surgery. J Craniofac Surg. 2015 May;26(3):906-10. DOI: 10.1097/SCS.0000000000001603
[42] Knize DM. Anatomic concepts for brow lift procedures. Plast Reconstr Surg. 2009 Dec;124(6):2118-26. DOI: 10.1097/PRS.0b013e3181bd0726
[43] Liebman EP, Webster RC, Berger AS, DellaVecchia M. The frontalis nerve in the temporal brow lift. Arch Otolaryngol. 1982 Apr;108(4):232-5. DOI: 10.1001/archotol.1982.00790520032009
[44] Ridgway JM, Larrabee WF. Anatomy for blepharoplasty and brow-lift. Facial Plast Surg. 2010 Aug;26(3):177-85. DOI: 10.1055/s-0030-1254327

